
CATHERINE RAMPELL
Dollars to doughnuts.
I’ve written recently about the job prospects for college graduates versus those without bachelor’s degrees, noting that the unemployment rate for college graduates is about half that for workers with no more than a high school diploma (3.7 percent versus 8.1 percent as of January). Several readers wrote me to take issue with the fact that I was looking at the whole universe of workers with these credentials, rather than just the recently graduated. Perhaps college graduates from generations past are more protected than those just entering the work force, they wrote, and it is misleading to say that young graduates are equally secure.
It is true that young workers have higher unemployment rates than their older counterparts, at just about all levels of education. A recent report published by the Bureau of Labor Statistics on the job prospects of new college graduates, for example, found that as of October 2011, the graduates of the class of 2011 had an unemployment rate of 14 percent.
But that number refers to joblessness just a few months after graduation. If you look at all recent college graduates in their 20s, the unemployment rate drops sharply. It is especially impressive when compared with the jobless rate for all high school graduates in the same age group.
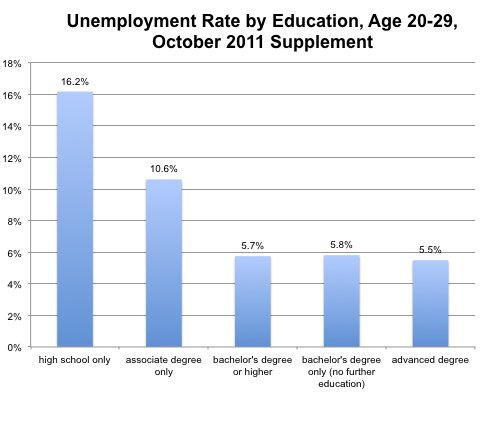 Sources: October School Enrollment Supplement, Current Population Survey, Bureau of Labor Statistics; Thomas Luke Spreen.
Sources: October School Enrollment Supplement, Current Population Survey, Bureau of Labor Statistics; Thomas Luke Spreen.
As you can see, the unemployment rate for people in their 20s with college degrees or more education was 5.7 percent (for those whose highest credential was no more than a bachelor’s, the number was 5.8 percent). For those with only a high school diploma or G.E.D., it was more than twice as high, at 16.2 percent.
Here are comparable numbers for the employment-population ratio, or the share of people within each population who have a job (as opposed to being unemployed or not looking for work at all).
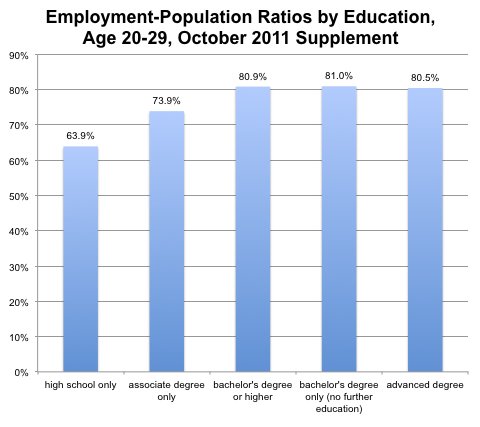 Sources: October School Enrollment Supplement, Current Population Survey, Bureau of Labor Statistics; Thomas Luke Spreen.
Sources: October School Enrollment Supplement, Current Population Survey, Bureau of Labor Statistics; Thomas Luke Spreen.
The data are from Thomas Luke Spreen, who wrote the Labor Department report mentioned above. His numbers are culled from the 2011 October School Enrollment Supplement, an annual supplement to the Current Population Survey. (The Bureau of Labor Statistics’ public data on unemployment by educational attainment usually covers all workers 25 or older only, rather than narrower or younger ranges of workers.)
Of course, many of those college-educated 20-somethings are getting jobs that don’t really require college-level skills. But at least they’re finding work, unlike their less-educated peers. And as the economy continues to improve, those recent college graduates will be better situated to find promotions to jobs that do use their higher skills and pay better wages.
Article source: http://economix.blogs.nytimes.com/2013/03/05/yes-even-young-college-graduates-have-low-unemployment/?partner=rss&emc=rss
